Maternal well-being outcomes in the United States continue to deteriorate, with maternal and infant mortality rates far exceeding those in Europe and other wealthy countries. Currently, another review driven by analysts at the Boston College School of General Wellbeing (BUSPH) and Harvard Clinical School-partnered Beth Israel Deaconess Clinical Center (BIDMC) is shedding knowledge on how clinic hierarchical designs and staffing inside US maternity care might influence the birthing system and perhaps add to unfriendly birth results.
Distributed in the journal PLOS ONE, the review examined gestational age examples and timing of home and clinic births in three top-level salary nations: the US, which embraces a maternity care model that depends vigorously on obstetricians and clinical mediations, and Britain and the Netherlands, which basically depend on birthing assistants who give low-mediation maternity care.
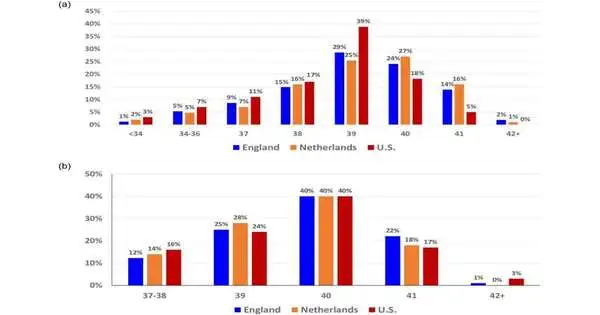
Overall, they are more limited than pregnancies in Britain and the Netherlands. In 2020, only 23% of US births occurred at least 40 weeks, compared to 44% of births in the Netherlands and 40% of births in the United Kingdom. The gestational age design for home births was similar in each of the three nations.
“Our multi-country analysis reveals that the United States is an outlier in terms of gestational age distribution and the time of low-intervention hospital births,”
Dr. Eugene Declercq, professor of community health sciences at BUSPH.
In each of the three countries, the researchers analyzed birth timing by hour of the day for homebirths and clinic-based vaginal births, and then repeated the analysis, limiting the correlation to clinic-based vaginal births without mediations, for example, acceptance or work expansion, that might actually change the timing.
In Britain and the Netherlands, births at home and at the clinic happened at comparable times in the day, peaking in the early morning hours between 1 a.m. and 6 a.m.
Yet, in the US, there was an observable contrast in birth timing between the two settings: births at home occurred in similar early morning hours as home births in different nations. Conversely, clinic-based births—even those without any mediations that could influence the normal example of timing—generally happen during standard working hours for clinical staff, from 8 a.m. to 5 p.m.
The paper is the main global review, utilizing huge datasets to look at gestational age and birth timing in three top-level salary nations; most earlier examinations have zeroed in on information from individual clinics or nations. Given Britain’s and the Netherlands’ unrivaled birthing results, the creators say their discoveries suggest the US maternity care models could profit from a hierarchical shift that puts less emphasis on dynamic, clinical administration of work and permits the birthing system to take on a normal flow.
“Our multi-country examination shows that the US is an exception in gestational age conveyance and timing of low-mediation clinic births,” says concentrate on lead and relating creator Dr. Eugene Declercq, teacher of local area wellbeing sciences at BUSPH. “There’s an example to be gained from nations with more sure maternity results than the US in having clinic staffing and functional plans adjust more near the normal examples of birth timing and gestational age as opposed to attempting to have birth timing fit hierarchical necessities.”
The review included broadly agent-based and freely accessible populace-based birth information from each of the three nations, remembering information for more than 3.8 million births in the US and 156,000 births in the Netherlands in 2014, and in excess of 56,000 births in Britain from 2008–2010. The analysts analyzed home and clinic birth timing for births that happened somewhere in the range of 37 and 42 weeks.
“Each framework is impeccably intended to achieve the outcomes that it achieves,” says focus on senior creator Dr. Neel Shah, the Expert Center’s chief clinical official and a meeting researcher at BIDMC. “The alarmingly unfortunate aftereffects of the US maternal wellbeing framework” request more prominent regard for its plan. “Our review shows that in comparison with other big-salary nations, American clinics might be intended to focus on the comfort of clinicians more than the necessities of individuals conceiving an offspring.”
More information: Eugene Declercq et al, The natural pattern of birth timing and gestational age in the U.S. compared to England, and the Netherlands, PLOS ONE (2023). DOI: 10.1371/journal.pone.0278856
Journal information: PLoS ONE




